

To overcome the gaps in diagnostic tests and difficulties in clinical diagnosis of childhood tuberculosis, several point scoring systems and diagnostic algorithms were previously developed. Historically, scores assigning numerical values to clinical characteristic, have been proposed by experts, aiming to standardize tuberculosis diagnosis.
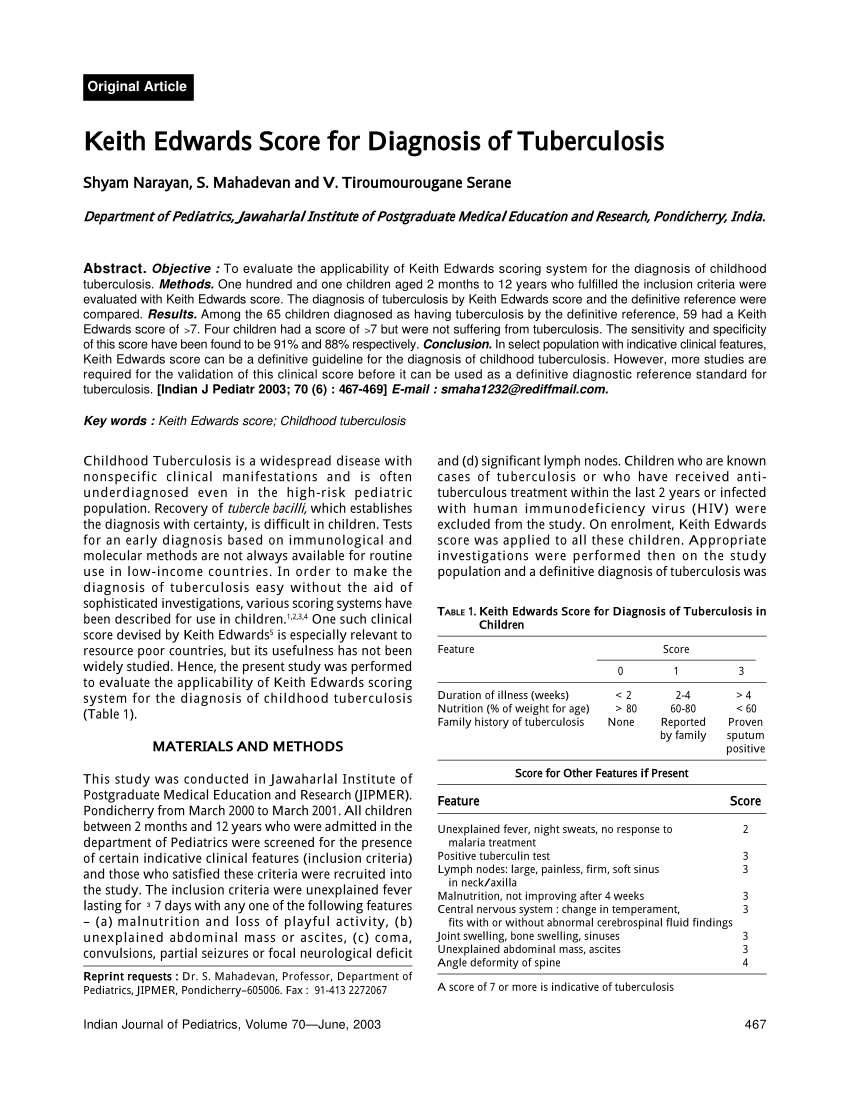
Three main scores have been developed and used: the Kenneth Jones/Stegen Toledo system, published in 1969 in Chile, the Keith Edwards criteria, originally published in 1987 in Papua New Guinea, , and finally, the Brazil Ministry of Health System. These historical scores were developed based on expert opinion, were heterogeneous, did not have a good diagnostic performance in HIV-infected children or malnourished children that are more vulnerable to TB, and were not validated.
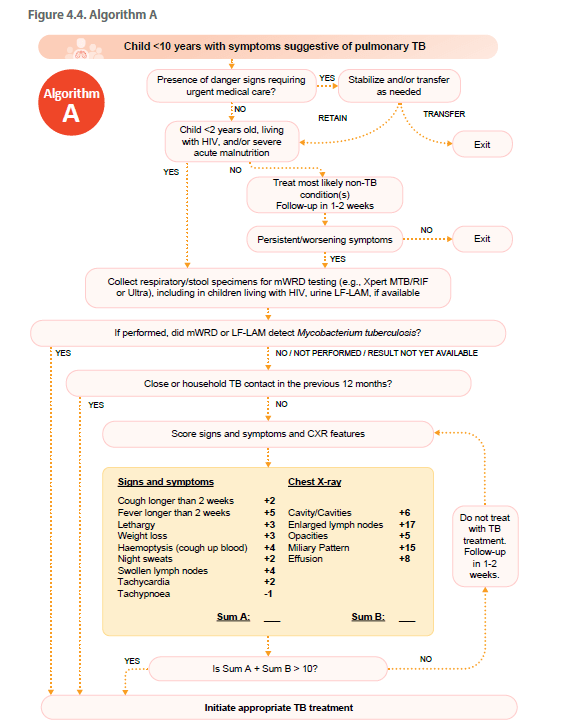
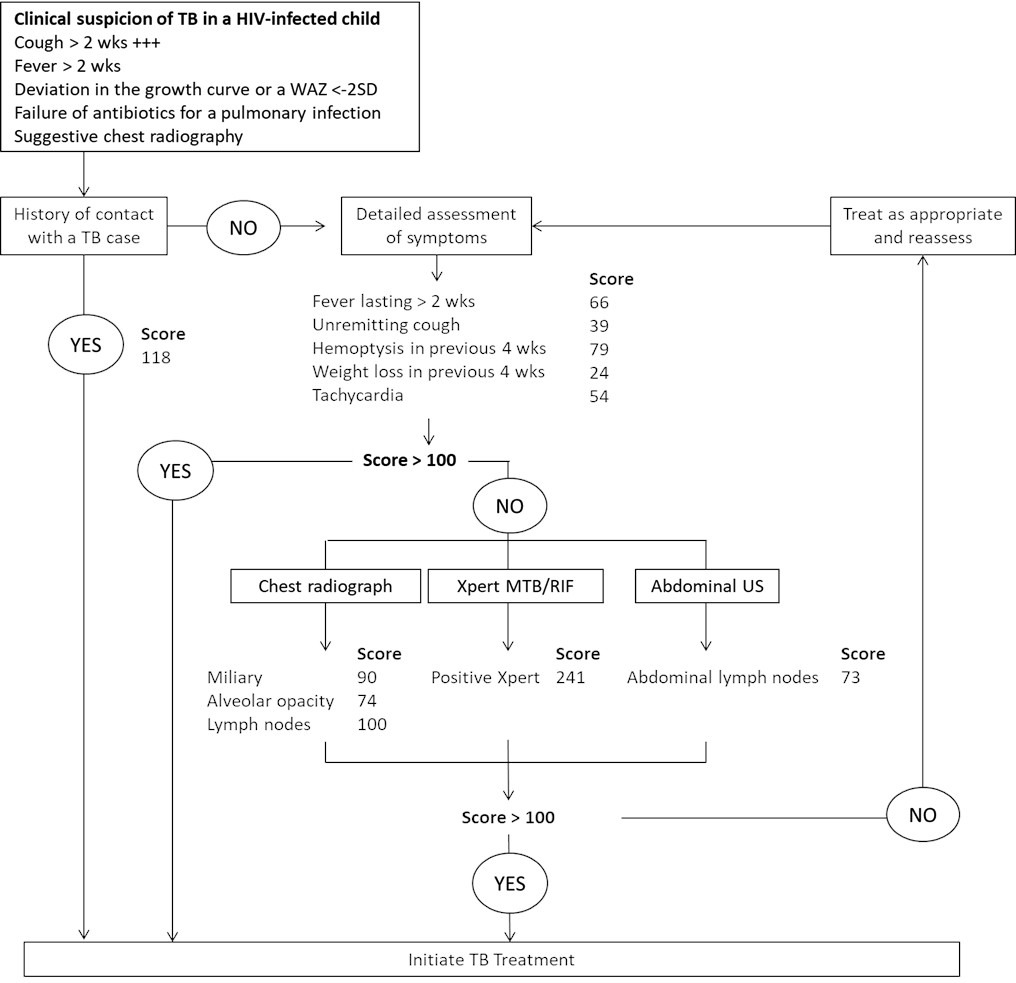
Due to these problems, original scores were not recommended by the WHO. The Union desk guide algorithm provided guidance on clinical TB diagnosis using algorithmic approach adapted to the HIV-status.

{kind=link}
{kind=link}
{kind=link}